AIIMS PG Entrance May 2006 [ Answers ]
AIIMS PG Entrance May 2006 [ Answers ]
1. (4)
Allodynia:
Cutaneous allodynia is the perception of pain produced by innocuous stimulation of normal skin and may result from sensitization of central pain pathways in migraine.
Ref: An association between migraine and cutaneous allodynia. Burstein R; Yarnitsky D; Goor
-Aryeh I; Ransil BJ; Bajwa ZH Ann Neurol 2000 May;47(5):614-24.
2. (4)
Blood gas solubility coefficient:
Agent Blood/gas (adults)
Halothane 2.57
Enflurane 1.91
Isoflurane 1.38
Sevoflurane 0.68
Desflurane 0.42
Nitrous Oxide 0.40
Ref:
1. Goodman – Gilman 10/E 349/P
2. Values are summarized from: Malviya, Anesthesiology 1990, Lerman J, Pharmacology of inhalational anesthetics in infants and children. Paediatric Anaesthesia 1992;2: 191-203.
Lerman J, Anesthesiology 1986.
3. (3)
Neuromuscular blocking agent with shortest onset of action:
Some confusion in this one:
Dose Onset
(mg/kg) (Sec)
Succinylcholine 1.0 51
Rapacuronium 1.5 54
Ref: Hayes A, Breslin D, Reid J, Mirakhur RK. Comparison of recovery following rapacuronium with and without neostigmine and succinylcholine. Anaesthesia 2000; 55: 859–63.
Succinylcholine 1.5 68
Rapacuronium 2.5 67
Ref: Abouleish EI, Abboud TS, Bikhazi GJ, et al. Rapacuronium for modified rapid sequence induction in elective Caesarean section: neuromuscular blocking effects and safety compared with succinylcholine, and placental transfer. Br J Anaesth 1999; 83: 862–7.
4. (1)
Administration of Glucose is prescribed in all except:
Since I feel that 'child to a diabetic mother' will already have hyperglycemia, a glucose solution administration will have no meaning. But I was wrong, because according to the Pedersen hypothesis, intermittent maternal hyperglycemia causes fetal hyperglycemia, which leads to premature maturation of fetal pancreatic islets, with hypertrophy of the beta cells and resultant hyperinsulinemia.
So I guess the answer is "Neonates".
Ref: PEDERSEN, J. Weight and length at birth of infants of diabetic mothers. Acta Endocrinol
(Copenh) 1954; 16:330.
5. (3)
Brain tumor is highly vascular in nature:
I guess the answer is "C P Angle epidermoid". Cerebellopontine (C P) angle tumor can be acoustic neuroma, meningioma, neurinoma of Vth or VIIth nerve, glomus jugulare tumor, dermoid, epidermoid cyst and Choroid Plexus Tumors. Out of them Choroid Plexus tumor and glomus jugulare tumor are highly vascular.
Ref:
1. Furuya et al. Primary Large Choroid Plexus Papillomas in the Cerebellopontine Angle:
Radiological Manifestation and Surgical Management. Acta Neurochirur ( Wien ) 136: 144-149;
1995.
2. Swenson MR, Sibley W. Glomus jugulare tumor. Postgrad Med. 1982 Aug;72(2):213–214.
6. (4)
Cranial nerves present in posterior fossa:
I thought the answer was 3rd - 12th Cr. N.
But I was wrong!
VI comes from the brain stem which lies in posterior fossa
Internal acoustic meatus: VII, VIII
Jugular Foramen: IX, X, XI
Anterior condylar (hypoglossal) canal: XII
- Dr. Anubhav Vindal(S.R. Surgery, MAMC).
7. (4)
Drugs used in managing status epilepticus:
The main categories of drugs used to treat SE are
1. benzodiazepines (example: diazepam)
2. phenytoin (or fosphenytoin)
3. barbiturates
4. propofol
5. valproic acid
Ref: Freeman, JM. Status epilepticus: it's not what we've thought or taught. Pediatrics 1989; 83:444.
Note: Some people say carbamazepine is less efficacious or less well studied and should not be considered part of the routine management of status epilepticus.
Some centers use thiopental (Thiopentone Sodium) instead of pentobarbital for refractory status epilepticus, but there are a number of problems with this approach. Animal studies suggest that thiopental carries a higher incidence of adverse cardiovascular effects than pentobarbital. The half-life of thiopental is shorter than that of pentobarbital, but this is counterbalanced by the fact that thiopental is degraded to active metabolites (including pentobarbital), which accumulate with longer term infusions. Thiopental may also have immunosuppressive effects on neutrophil function and mucociliary clearance.
Ref:
1. The intensive care treatment of convulsive status epilepticus in the UK. Results of a
national survey and recommendations. Walker MC; Smith SJ; Shorvon SD
Anaesthesia 1995
Feb;50(2):130-5.
2. Intravenous anesthetics and human neutrophil granulocyte motility in vitro Kress HG;
Segmuller R Anaesthesist 1987 Jul;36(7):356-61.
3. Depression of lung mucociliary dlearance by thiopental and halothane. Forbes AR; Gamsu G
Anesth Analg 1979 Sep-Oct;58(5):387-9.
So I am confused whether one should tick Carbamazepine or Thiopental? But it seems like that the former is the correct answer.
8. (3)
Cushing's Triad
A triad of:
1. bradycardia
2. respiratory depression
3. hypertension
is called Cushing's triad (sometimes called Cushing's reflex or Cushing's response).
While the mechanism of Cushing's triad remains controversial, many believe that it relates to brainstem compression. The presence of this response is an ominous finding that requires urgent intervention.
Ref: Kaye, AH. Brain Tumors: An Encyclopedic Approach, 2 ed, Churchill Livingstone, New
York, 2001:205.
9. (4)
Systemic secondary injury to brain:
Well Hypothermia to certain extent protects brain by reducing metabolic processes, so it
(Looking at other options) is not logical that it might play a major role in injuring it.
10. (4)
Neostigmine antagonizes
Ref: KDT 3/E 86/P
11. (1)
Ref: Ganong 17/e 609/p
12. (4)
All of the following is used for treating hyperkalaemia,
1. Calcium gluconate
2. Sod. bi carb.
3. intravenous infusion of glucose with insulin
Intracellular movt of potassium is mediated by beta adrenergic receptors…so beta blockers stop this movt and raise serum potassium levels
- Dr. Vaibhav Sahni (S.R. Medicine, MAMC)
13. (1)
Ref: Harrison’s 16/e 1825/p
14. (1)
Coronary blood flow:
directly related to perfusion pressure and inversely related to resistance just like any blood flow pressure increases and resistance decreases flow.
- Dr. Vaibhav Sahni
15. (1) ?
Most significant adverse effect of ACE inhibitor is:
1. Hypotension
2. Hypertension
3. Hypocalcaemia
4. Hypercalcaemia rate answer is hyperkalemia
I don’t understand what hypercalcemia rate means. ACE inhibitors cause hypotension but very rarely…they may however cause first dose hypotension sometimes. Hypocalcemia or hypertension is not possible
- Dr. Vaibhav Sahni
16. (2)
Ref: KDT 3/e 207/p
17. (4)
Ref: KDT 5/e 164/p
18. (2)
- Dr. Anubhav Vindal
19. (1)
- Dr. Anubhav Vindal
20. (1)
- Dr. Anubhav Vindal
21. (3)
- Dr. Anubhav Vindal
22. (3)
A 40 yr old female patient presented with dysphagia to both liquids and regurgitation solids and for 3 months the dysphagia was non progressive, what is the most likely diagnosis is Achalasia cardia because dysphagia to both liquids nad solids suggests a motility disorder, not a structural one
- Dr. Vaibhav Sahni
23. (4)
- Dr. Ashwini Sethi (S.R. E.N.T., MAMC)
24. (3)
A 15 yr old boy presented with 1 d history of bleeding gum, subconjuctival bleed and the purpuric rash. Investigation revealed the following results:
Hb-6.4, TLC-26,500, Platelets-35,000,PT-20s with control of 13s, PTT-50s and fibrinogen 10mg/dl. Peripheral smear suggestive of AML. What is the most probable diagnosis?
Investigations suggests disseminated intravascular coagulopathy (DIC) – a typical presentation of promyelocytic leukemia.
- Dr. Vaibhav Sahni
25. (1)
Ref: Saini 2/e 7.5/p
26. (3)
Ref: Saini 2/e 6.26/p
27. (2)
pH=-log[H+]
28. (3)
Ref: Saini 2/e 9.71/p
29. (3)
Ref: Ananthnarayan 5/e 286/p
30. (2)
Homocysteine is an a.a. associated with Atherosclerosis
Ref: Kilmer McCully: pioneer of the homocysteine theory. Lancet 1998 352: 1364.
31. (4)
Ref: Robbin’s 5/e 300/p
32. (3) ?
Most of the searches landed me up into Hydrogen peroxide being a second messenger [Plant Cell, Vol. 13, 179-191, January 2001, Copyright © 2001, American Society of Plant Physiologists, Hydrogen Peroxide Acts as a Second Messenger for the Induction of Defense Genes in Tomato Plants in Response to Wounding, Systemin, and Methyl Jasmonate Martha L. Orozco-Cárdenasa, Javier Narváez-Vásqueza, and Clarence A. Ryana ].
Amongst the examples, I feel it should be Calcium. The article [Published 5 July 2004. doi:10.1083/jcb.200310145 JCB, Volume 166, Number 1, 111-119 Extracellular calcium acts as a "third messenger" to regulate enzyme and alkaline secretion, Rosa Caroppo1, Andrea Gerbino1, Gregorio Fistetto1, Matilde Colella1,2, Lucantonio Debellis1, Aldebaran M. Hofer2, and Silvana Curci1,2] says it acts as third messenger but if we take the definition, "Second messengers are molecules that relay signals received at receptors on the cell surface — such as the arrival of protein hormones, growth factors, etc. — to target molecules in the cytosol and/or nucleus. " then Calcium becomes an important Secondary messenger.
33. (2)
A != T && C != G
34. (4)
This is a debatable question though, because we never know how a mutation in intronic region affect the whole process (it might be a regulatory region or a splice site controller?) Anyways since we are appearing in medical entrance and not biotechnology one, we can safely go for the option (4)!
35. (1)
Ref: Park 18/e
36. (3)
Ref: Park 18/e 651/p
37. (3)
We are asked here to calculate the Negative predictive value.
[(Not Diseased)*(Specificity)]/[(Not Diseased)*(Specificity)
+ (Diseased)*(1-Sensitivity)]
[70*0.8]/[70*0.8+30(1-0.9)] =~ 95%
Ref: Harrison’s 14/e 10/p
38. (4)
Ref: Mahajan 6/e 11/p
39. (2)
Ref: Park 14/e 482/p
40. (1)
Ref: Park 14/e 480/p
41. (4) ?
Ref: Park 14/e 37/p
42. (4)
Ref: Ananthnarayan 5/e 481/p
43. (1)
Ref: Ananthnarayan 5/e 320/p
44. (2)
Ref: Ananthnarayan 5/e 320/p
45. (2)
Ref: Park 14/e 406/p
46. (2)
Ref: Park 18/e 241/p
47. (1)
48. (3)
Dr. Puneet Setia (S.R. Forensic Medicine, PGI Chandigarh)
49. (4)
Dr. Rahul Malhotra (S.R. Pulic Health, MAMC)
50. (1)
Ref: CMDT 2000/y 197/p
51. (2)
Ref: Park 14/e 347/p
52. (4)
Ref: Park 14/e 350/p
53. (4)
Ref: Park 14/e 15/p
54. (1)
Ref: Ananthnarayan
55. (4)
Ref: Park 14/e 111/p
56. (1)
Ref: Taber’s medical dictionary
57. (1)
Chancre redux I found out is another name for early relapse of syphilis
- Dr. Vaibhav Sahni
58. (2)
Max Joseph's space is linked to Lichen Planus.
Ref: Phd thesis of Laeijendecker, Proefschr on Lichen Planus.
59. Ivermectin is used in treating Scabies.
Ref: Prescrire Int. 2002 Oct;11(61):137-40; Ivermectin: new indication. Oral treatment of scabies: simple and effective.
60. (2)
Ref: Harrison’s 14/e 1016/p
61. (1)
Following is not used for treatment of typeII lepra reaction:
1. Chloroquin
2. Thalidomide
3. Cyclosporine
4. Corticosteroids
All others have an anti-inflammatory action and are used
- Dr. Vaibhav Sahni
62. (1)
Lepramin test is a test to measure cell mediated immunity. It just suggest whether the pt is immunocompetent or not. A lepramin negative pt develops the severe lepromatous leprosy and a lepramin positive one develops tuberculoid leprosy. This test cannot be used to diagnose leprosy.
- Dr. Vaibhav Sahni
63. (2)
Ref: Harrison’s 14/e 298/p
64. (2)
Ref: Maheshwari 3/e 81/p
65. (2)
Presentation suggests mononeuritis multiplex, nephritic syndrome , a young male----all typical of PAN
- Dr. Vaibhav Sahni
66. (4)
All of the following is used for giving traction, EXCEPT:
>1. Steinmann's Pin
>2. Kirschner's Wire
>3. Bohler's Stirrup
>4. Rush Pin*
- Dr. Ankur Gupta (S.R. Orthopaedics, RML)
67. (4)
All of the following are compilation of supracondylar fracture of
>humerus in children, except:
>1. Compartment syndrome
>2. Myositis ossificans
>3. Malunion
>4. Non union*
- Dr. Ankur Gupta
Ref: Maheshwari 2/e 84/p
68. (4)
Lesion associated with recurrent dislocation of shoulder include all,
>EXCEPT:
>1. Hill-Sach's lesion
>2. Bankart's lesion
>3. Capsular laxity
>4. Supraspinatous tear*
- Dr. Ankur Gupta
Ref: Maheshwari 2/e 74/p
69. (4)
All of the following are the cause of sudden increase in pain in
>osteochondroma, except:
>1. Sarcomatous change
>2. Fracture
>3. Bursitis
>4. Degenerative changes*
70. (3)
Dr. Anubhav Vindal
71. (2) ?
# The upper division of the oculomotor nerve (cranial nerve III) innervates the superior rectus and the levator palpebrae superioris muscles.
# The lower division of cranial nerve III innervates the inferior rectus, medial rectus, and inferior oblique muscles. The nerve to the inferior oblique muscle enters the muscle laterally at the junction of the inferior oblique and inferior rectus muscles.
# The trochlear nerve (cranial nerve IV) supplies the superior oblique muscle. The nerve to the superior oblique muscle enters the muscle approximately one third of the distance from the origin to the trochlea.
# The abducens nerve (cranial nerve VI) supplies the lateral rectus muscle.
# The parasympathetic innervation to the pupillary sphincter and ciliary muscle travels with the nerve to the inferior oblique muscle. The parasympathetics may be injured during inferior oblique surgery or orbital floor surgery.
Ref: http://www.emedicine.com/neuro/topic636.htm
And http://anesthesiologyinfo.com/articles/12092002.php says that “Retrobulbar block is aimed at blocking the ciliary ganglion, ciliary nerves, and cranial nerves II, III and VI. Cranial nerve IV is not affected since it lies outside the muscle cone. When the block is performed, the local anesthetic is delivered within the muscle cone itself.”
If we combine the above two we can see that superior oblique supplied by Cr. N. IV will not be much affected.
72. (2) or (4)?
For PHPV, prognosis is usually not good.
Ref: Trans Am Ophthalmol Soc. 1997;95:487-549. Persistent hyperplastic primary vitreous: diagnosis, treatment and results. Pollard ZF.
But one of my friend says answer can be (4) also, because it is asssosiated with microphthalmos.... not exophthalmos
- Dr. Pankaj Mehta
73. (3)
Panretinal photocoagulation is used for treating iris neovascularisation.
Ref: Ophthalmology. 1981 Nov;88(11):1102-6. A grading system for iris neovascularization. Prognostic implications for treatment.
74. (1)
- Dr. Pankaj Mehta
75. (2)
Ref: Neema 3/e 292/p
76. (3)
Ref: Robbin’s 5/e 236/p
77. (3)
Ref: Khurana 1/e 194/p
78. (2)
Ref: Khurana 1/e 144/p
79. (3)
Ref: Khurana 1/e 288/p
80. (2)
Ref: Khurana 1/e 289/p
81. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
82. (2)
Ref: Parikh 5/e 146/p
83. (2) ?
Dr. Anubhav Vindal
84. (4)
Ref: Reddy 16/e 146/p
85. (1)
Ref: Reddy 16/e 66/p
86. (1)
Ref: Reddy 24/e 125/p
87. (3)
Ref: Reddy 16/e 452/p
88. (4)
Ref: Robbin’s 5/e 1058/p
89. (4)
Ref: Harrison’s 14/e 2106/p
90. (4) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
91. (1)
- Dr. Anubhav Vindal
92. (3)
- Dr. Neeraj Srivastava (Resident CUNY, NYC) and Dr. Rachna Srivastava
93. (2)
Ref: Shaw’s 12/e 315/p
94. (2) ?
PREGNANCY INDUCED HYPERTENSION
37 WEEKS
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
95. (4) ?
ASHERMAN SYNDROME
(MISSED ABORTION)
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
96. (1) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
97. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
I think it is because of reflex hyperinsulinemia in the fetus because of hyperglycemia in mother…
98. (4) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
99. (3)
Propofol . It is the recommended day care anaesthetic agent because of
Smooth induction , anti emetic and anti pruritic quality and smooth and
Pleasant clear headed recovery . The added mtp conundrum is a distraction at
Best .
Dr. Kapil Arya (S.R. Anaesthesia, LHMC)
100. (1)
- Dr. Neeraj and Rachna Srivastava
101. (4)
- Dr. Ashwini Sethi
102. (1)
- Dr. Ashwini Sethi
103. (2) ?
- Dr. Ashwini Sethi
But there is some controversy here as Harrison’s 14/e 2379/p puts Vertigo not as a typical feature.
104. (3)
- Dr. Ashwini Sethi
Ref: Harrison’s 14/e 944/p.
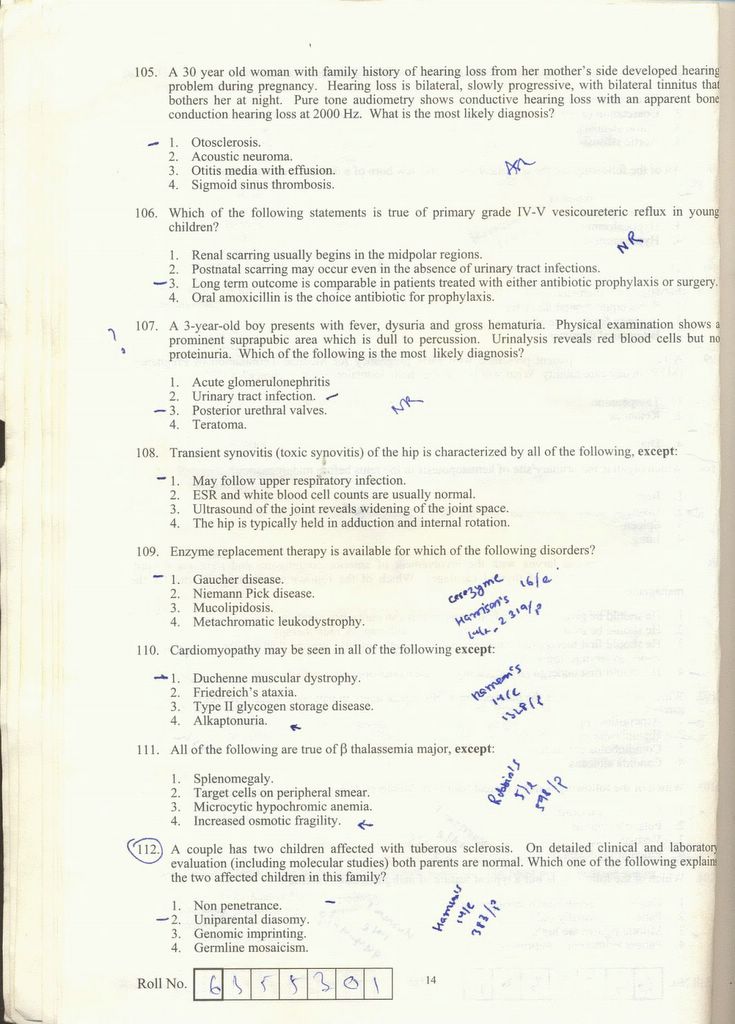
105. (1)
- Dr. Ashwini Sethi
106. (3)
- Dr. Neeraj and Rachna Srivastava
107. (2) ?
- Dr. Neeraj and Rachna Srivastava
But there is some controversy here because some of my friends say it is (3) Posterior urethral valve.
108. (1) ?
Transient synovitis (toxic synovitis) of the hip is characterized by all of the following, except:
4. The hip is typically held in adduction and internal rotation.
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
109. (1)
Ref: Harrison’s 14/e 2319/p
110. (4)
Ref: Harrison’s 14/e 1328/p
111. (4)
Ref: Robbin’s 5/e 598/p
112. (1)
Ref: Harrison’s 14/e 383/p
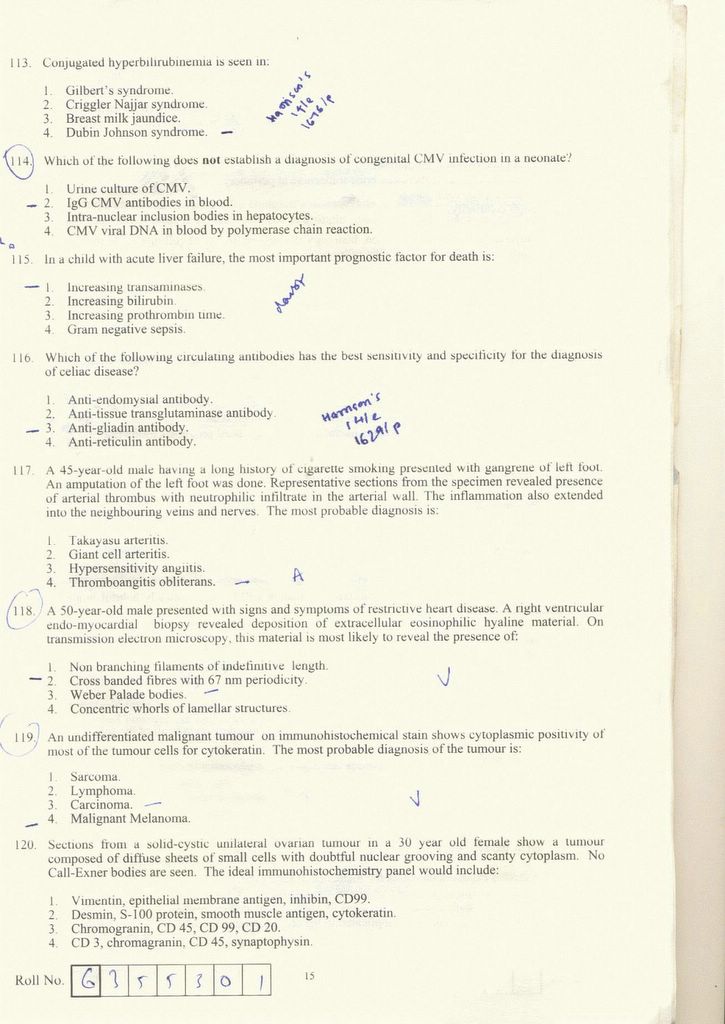
113. (4)
Ref: Harrison’s 14/e 1676/p
114. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
115. (4)
MAY BE 4 PROGNOSIS IN ARF DEPEND ON UNDERLYING Ds....BETTER WITH PRERENAL CAUSE THAN RENAL AND POST RENAL…
- Dr. Neeraj and Rachna Srivastava
116. (3)
Ref: Harrison’s 14/e 1629/p
117. (4)
- Dr. Anubhav Vindal
118. (3)
This is a case of amyloidosis.
- Dr. Vaibhav Sahni
119. (3)
Cytokeratin is an epithelial tissue marker. Only a carcinoma originates from epithelium.
- Dr. Vaibhav Sahni
120. (3) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
121. (3)
Ref: Robbin’s 5/e 1238/p
122. (4)
A differential diagnosis of lesion, histologically resemblin giant cell
>tumor in the small bones of hands or feet inclused all of the following
>EXCEPT:
>1. Aneurysmal bone cyst
>2. Fibrosarcoma
>3. Osteosarcoma
>4. Hyperparathyroidism*
- Dr. Ankur Gupta
123. (2)
Ref: Khurana 1/e 278/p
124. (1)
- Dr. Pankaj Mehta
125. (1) or (3)
Ref: Robbin’s 5/e 598/p says (1)
- Dr. Neeraj and Rachna Srivastava say (3)
126. (4)
- Dr. Neeraj and Rachna Srivastava
127. (2)
- Dr. Neeraj and Rachna Srivastava
128. (3)
46 XXY
Ref: Robbin’s 5/e 159/p
129. (4)
Ref: Robbin’s 5/e 635/p
130. (4)
Ref: Robbin’s 14/e 704/p
131. (3)
Acute leukemias show blasts in peripheral smear. Basophilia is a characteristic feature of CML.
- Dr. Vaibhav Sahni
132. (2)
Hb is normal so polycythemia is out. Normal TLC rules out leukemoid rxn. Also, this doesn’t suggest CML. Though platelets are only mildly raised I would still put my money behind thrombocythemia.
- Dr. Vaibhav Sahni
133. (3)
A 70 yr old with pathological fracture of femur. The lesion appears
>lytic on X-Ray film with a circumscribed punched out appearance. The
>curetting from the fracture site is most likely to show which of the
>following:
>1. Diminished and thinned trabecular bone fragments secondary to osteopenia
>2. Sheets of atypical plasma cells
>3. Metastatic prostatic adenocarcinoma*
>4. Malignant cell forming osteoid bone
- Dr. Ankur Gupta
134. (2)
Angiocentric lymphoma is a T-Cell lymphoma.
Ref: Journal of Clinical Pathology 2005;58:550-552 2005 BMJ Publishing Group Ltd & Association of Clinical Pathologists: Angiocentric immunoproliferative lesion and angiocentric lymphoma of lymph node in children. A report of two cases: R Drut and R M Drut.
135. (1)
Ref: Robbin’s 5/e 1137/p
136. (1)
Ref: Harrison’s 14/e 1593/p
137. (2)
It is a Vit K congener.
Ref: Harrison’s 14/e 745/p
KDT 3/e 544/p
138. (4)
- Dr. Divakar Sharma (S.R. Anesthesia, Safdarjung)
139. (2)or (4)
- Dr. Kapil Arya says (3)
Ref: KDT 3/e 315/p says (4)
140. (4)
- Dr. Kapil Arya says (3)
141. (1)
Ref: KDT 3/e 765/p
142. (1)
Imatinib inhibits Tyrosine kinase.
Ref: PNAS | September 20, 2005 | vol. 102 | no. 38 | 13622-13627: The kinase inhibitor imatinib mesylate inhibits TNF-{alpha} production in vitro and prevents TNF-dependent acute hepatic inflammation: Anna Maria Wolf , Dominik Wolf, Holger Rumpold, Susanne Ludwiczek, Barbara Enrich, Guenther Gastl, Guenter Weiss, and Herbert Tilg.
143. (2)
Letrozole is an aromatase inhibitor.
Ref: J Clin Oncol. 1998 Feb;16(2):453-61. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: double-blind randomized trial showing a dose effect and improved efficacy and tolerability compared with megestrol acetate. Dombernowsky P, Smith I, Falkson G, Leonard R, Panasci L, Bellmunt J, Bezwoda W, Gardin G, Gudgeon A, Morgan M, Fornasiero A, Hoffmann W, Michel J, Hatschek T, Tjabbes T, Chaudri HA, Hornberger U, Trunet PF.
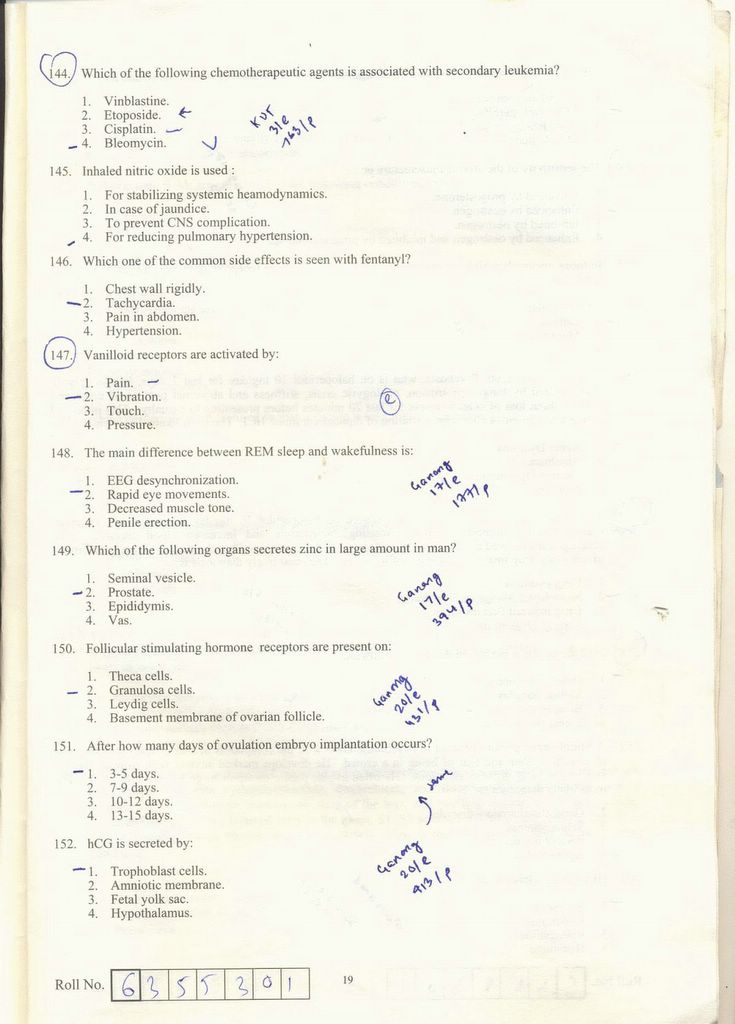
144. (3)
Secondary leukemia is a common long term side effect of alkylating agents like cisplatin, doxorubicin, daunorubicin, idarubicin etc…
- Dr. Vaibhav Sahni
145. (4)
FOR REDUCING PULMONARY HYPERTENSION . IT IS A MEDICINE QUESTION . NITRIC OXIDE IS NO . NITROUS OXIDE , N2O IS AN ANAESTHETIC AGENT.
- Dr. Kapil Arya
146. (1)
CHEST WALL RIGIDITY
- Dr. Kapil Arya
147. (1)
Vanilloid receptors are activated by Pain.
" Capsaicin functions in nociception by binding to a specific receptor, called the vanilloid receptor (Caterina et al., 1997). "
Ref: Caterina, M.J., Schumacher, M.A., Tominaga, M., Rosen, T.A., Levine, J.D., and Julius, D. The Capsaicin Receptor: a heat-activated ion channel in the pain pathway. Nature 389: 816-24 (1997)
148. (2)
Ref: Ganong 17/e 177/p
149. (2)
Ref: Ganong 17/e 394/p
150. (2)
Ref: Ganong 20/e 431/p
151. (1)
Ref: Ganong 20/e 413/p
152. (1)
Ref: Ganong 20/e 413/p
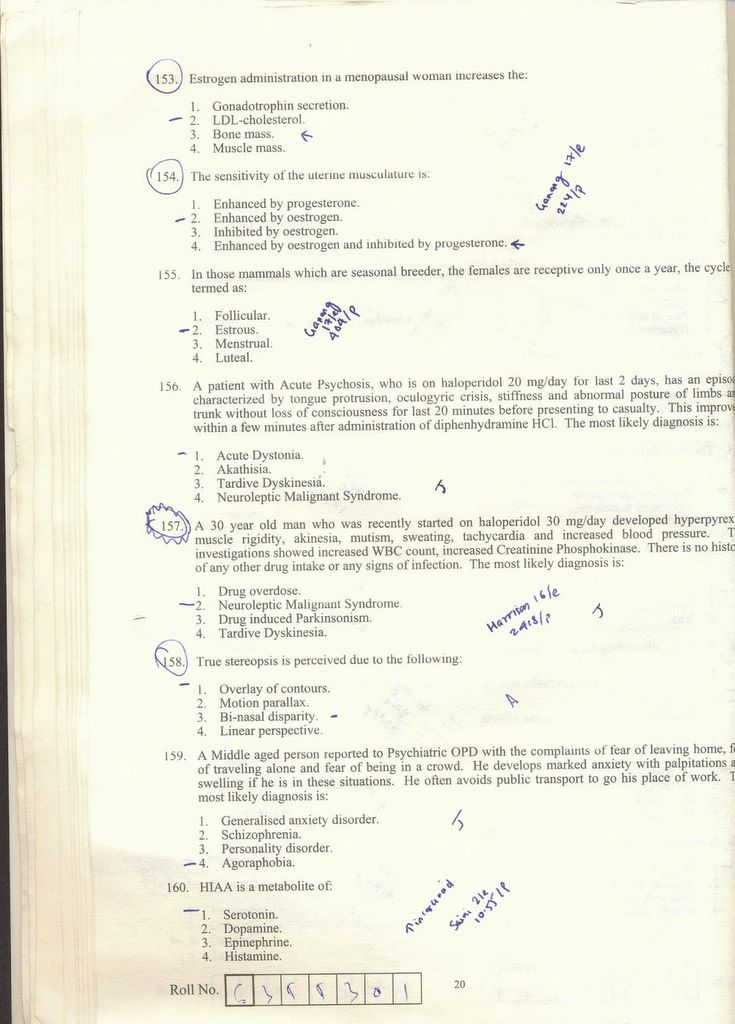
153. (4) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
154. (4)
Ref: Ganong 17/e 224/p
155. (2)
Ref: Ganong 17/e 404/p
156. (1)
Acute dystonia Sort of hypersenstivity to anti dopaminergic ( mostly all anti psychotics) that is why responds to diphenhydramine and no loss of consciousness.
- Dr. Jatan Parmar (Resident Psychiatry, UK)
157. (2)
Too much anti dopaminergic and due to this very high acetylcholine (see saw with dopamine in the motor control system) leading to muscular rigidity (actually leading to muscle breakdown and high CPK) and labile blood pressure ( inc. OR decrease) Life threatening emergency. Treatment includes supportive measures like controlling temp and blood pressure and also centrally acting muscle relaxants commonly Dantrolene intramuscularly.
- Dr. Jatan Parmar
158. (3)
- Dr. Anubhav Vindal
Ref: Harrison’s 14/e 161/pn
159. (4)
Agoraphobia ( which actually means fear of open spaces) includes fear and subsequent avoidance of crowded places like public transport. It can be with or without panic disorder, in this case it is classically described with it.
- Dr. Jatan Parmar
160. (1)
Ref: Saini 2/e 10.55/p
161. (1)
Ref: Ananthnarayan 5/e 574/p
162. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
163. (3) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
164. (3) ?
165. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
166. (4)
Blasts and mediastinal LN suggest childhood ALL which is a Bcell malignancy.
- Dr. Vaibhav Sahni
167. (2)
Presentation suggests CHF – a common complication of doxorubicin.
- Dr. Vaibhav Sahni
168. (1)
Nodular growth in sunexposed areas especially the face and pearly appearance is characteristic of basal cell carcinoma.
- Dr. Vaibhav Sahni
169. (3)
This is a presentation of pancoasts tumour- seen in mostly SCC, can also be seen in small cell ca. Adenocarcinoma is usually central and does not have this complication.
- Dr. Vaibhav Sahni
170. (2)
>A 15 yr old boy is injured while playing cricket. X-Ray of leg rule out
>a possible fracture. The radiologist reports the boy has and evidence of an
>agressive bone tumor with both bone destruction and soft tissue mass. The
>bone biopsy reveals a bone cancer with neural differentiation. Which of the
>following is most likely diagnosis:
>1. Chodroblastoma
>2. Ewing's sarcome*
>3. Neuroblastoma
>4. Osteosarcome
171. (2)
- Dr. Anubhav Vindal
172. (2) ?
173. (2)
Ref: Robbin’s 5/e 1137/p
174. (1)
Ref: NMS Anatomy 2/e 529/p
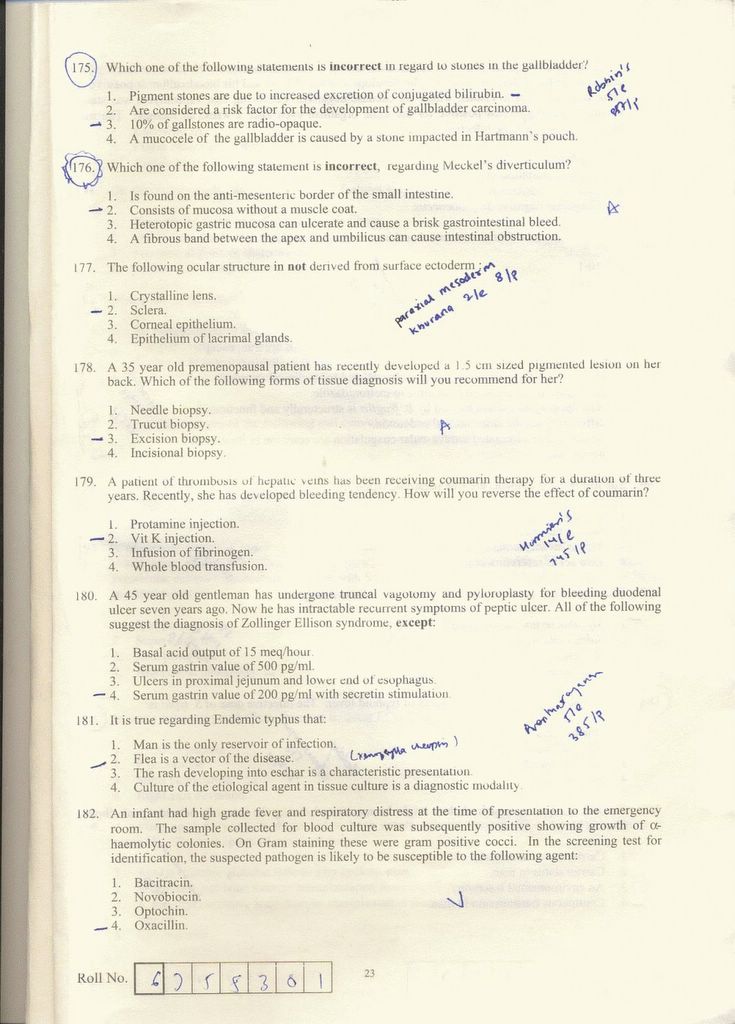
175. (1)
Ref: Robbin’s 5/e 857/p
176. (2)
- Dr. Anubhav Vindal
177. (2)
Ref: Khurana 1/e 8/p
178. (3)
- Dr. Anubhav Vindal
179. (2)
Ref: Harrison’s 14/e 745/p
180. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
181. (2)
Ref: Ananthnarayan 5/e 385/p
182. (4)
Gram positive cocci in clusters and alpha hemolysis suggests staph aureus. It is commonly resistant to penicillin group but sensitive to methicillin group i.e. oxacillin, cloxacillin, etc
- Dr. Vaibhav Sahni
183. (3)
Gram positive cocci in chains and catalase negative suggests streptococcus group. Now enterococcus is commonly resistant to most antibiotics in contrast to viridans and is a common cause of nosocomial sepsis in pts in ICU
- Dr. Vaibhav Sahni
184. (3)
Ref: Ananthnarayan 5/e 245/p
185. (4)
Ref: Harrison’s 14/e 995/p
186. (4)
Ref: Harrison’s 14/e 1036/p
187. (1)
Ref: Harrison’s 14/e 782/p
188. (2)
Ref: Ananthnarayan 5/e 272/p
189. (4)
Ref: Ananthnarayan 5/e 288/p
190. (3)
Ref: Ananthnarayan 5/e
191. (2)
No explanation for this , you have TO REMEMBER THE FEATURES OF DENERVATION AND OF MYOPATHY. Polyphasic waves is a feature of myopathy.
- Dr. Vaibhav Sahni
192. (1)
- Dr. Neeraj and Rachna Srivastava
193. (3)
Known side effect of topiramate……man no one knows why!
- Dr. Vaibhav Sahni
194. (4)
Ref: Reddy 16/e 425/p
195. (3)
All of these are ECG findings of PE. Sinus tachy is the earliest and most common sign. S1Q3T3 is the most specific.
- Dr. Vaibhav Sahni
196. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
197. (2)
This suggests acute polyneuropathy. Descending presentation is seen in botulism and diphtheria but papillary involvement is seen only in botulism
- Dr. Vaibhav Sahni
198. (3)
Weakness is seen in hypokalemia, hypocalcemia, hypomagnesemia, hypophosphatemia, hypercalcemia…not usually in sodium problems
- Dr. Vaibhav Sahni
199. (1)
Triphasic waves is a characteristic EEG pattern of hepatic enceph. Don’t ask me why!
- Dr. Vaibhav Sahni
200. (4)
Factor XIII action is to stabilize the clot formed initially. Fibrin lysis test is abnormal in its deficiency.
My Sincere thanks to Anubhav, Vaibhav, Neeraj, Rachna, Pankaj, Tulsi, Divakar, Kapil, Ashwini, Ankur, Puneet, Rahul, Jatan, Medical Books and The Internet!
- Ani
PS: The Scanned Question paper is available in the previous posting.
1. (4)
Allodynia:
Cutaneous allodynia is the perception of pain produced by innocuous stimulation of normal skin and may result from sensitization of central pain pathways in migraine.
Ref: An association between migraine and cutaneous allodynia. Burstein R; Yarnitsky D; Goor
-Aryeh I; Ransil BJ; Bajwa ZH Ann Neurol 2000 May;47(5):614-24.
2. (4)
Blood gas solubility coefficient:
Agent Blood/gas (adults)
Halothane 2.57
Enflurane 1.91
Isoflurane 1.38
Sevoflurane 0.68
Desflurane 0.42
Nitrous Oxide 0.40
Ref:
1. Goodman – Gilman 10/E 349/P
2. Values are summarized from: Malviya, Anesthesiology 1990, Lerman J, Pharmacology of inhalational anesthetics in infants and children. Paediatric Anaesthesia 1992;2: 191-203.
Lerman J, Anesthesiology 1986.
3. (3)
Neuromuscular blocking agent with shortest onset of action:
Some confusion in this one:
Dose Onset
(mg/kg) (Sec)
Succinylcholine 1.0 51
Rapacuronium 1.5 54
Ref: Hayes A, Breslin D, Reid J, Mirakhur RK. Comparison of recovery following rapacuronium with and without neostigmine and succinylcholine. Anaesthesia 2000; 55: 859–63.
Succinylcholine 1.5 68
Rapacuronium 2.5 67
Ref: Abouleish EI, Abboud TS, Bikhazi GJ, et al. Rapacuronium for modified rapid sequence induction in elective Caesarean section: neuromuscular blocking effects and safety compared with succinylcholine, and placental transfer. Br J Anaesth 1999; 83: 862–7.
4. (1)
Administration of Glucose is prescribed in all except:
Since I feel that 'child to a diabetic mother' will already have hyperglycemia, a glucose solution administration will have no meaning. But I was wrong, because according to the Pedersen hypothesis, intermittent maternal hyperglycemia causes fetal hyperglycemia, which leads to premature maturation of fetal pancreatic islets, with hypertrophy of the beta cells and resultant hyperinsulinemia.
So I guess the answer is "Neonates".
Ref: PEDERSEN, J. Weight and length at birth of infants of diabetic mothers. Acta Endocrinol
(Copenh) 1954; 16:330.
5. (3)
Brain tumor is highly vascular in nature:
I guess the answer is "C P Angle epidermoid". Cerebellopontine (C P) angle tumor can be acoustic neuroma, meningioma, neurinoma of Vth or VIIth nerve, glomus jugulare tumor, dermoid, epidermoid cyst and Choroid Plexus Tumors. Out of them Choroid Plexus tumor and glomus jugulare tumor are highly vascular.
Ref:
1. Furuya et al. Primary Large Choroid Plexus Papillomas in the Cerebellopontine Angle:
Radiological Manifestation and Surgical Management. Acta Neurochirur ( Wien ) 136: 144-149;
1995.
2. Swenson MR, Sibley W. Glomus jugulare tumor. Postgrad Med. 1982 Aug;72(2):213–214.
6. (4)
Cranial nerves present in posterior fossa:
I thought the answer was 3rd - 12th Cr. N.
But I was wrong!
VI comes from the brain stem which lies in posterior fossa
Internal acoustic meatus: VII, VIII
Jugular Foramen: IX, X, XI
Anterior condylar (hypoglossal) canal: XII
- Dr. Anubhav Vindal(S.R. Surgery, MAMC).
7. (4)
Drugs used in managing status epilepticus:
The main categories of drugs used to treat SE are
1. benzodiazepines (example: diazepam)
2. phenytoin (or fosphenytoin)
3. barbiturates
4. propofol
5. valproic acid
Ref: Freeman, JM. Status epilepticus: it's not what we've thought or taught. Pediatrics 1989; 83:444.
Note: Some people say carbamazepine is less efficacious or less well studied and should not be considered part of the routine management of status epilepticus.
Some centers use thiopental (Thiopentone Sodium) instead of pentobarbital for refractory status epilepticus, but there are a number of problems with this approach. Animal studies suggest that thiopental carries a higher incidence of adverse cardiovascular effects than pentobarbital. The half-life of thiopental is shorter than that of pentobarbital, but this is counterbalanced by the fact that thiopental is degraded to active metabolites (including pentobarbital), which accumulate with longer term infusions. Thiopental may also have immunosuppressive effects on neutrophil function and mucociliary clearance.
Ref:
1. The intensive care treatment of convulsive status epilepticus in the UK. Results of a
national survey and recommendations. Walker MC; Smith SJ; Shorvon SD
Anaesthesia 1995
Feb;50(2):130-5.
2. Intravenous anesthetics and human neutrophil granulocyte motility in vitro Kress HG;
Segmuller R Anaesthesist 1987 Jul;36(7):356-61.
3. Depression of lung mucociliary dlearance by thiopental and halothane. Forbes AR; Gamsu G
Anesth Analg 1979 Sep-Oct;58(5):387-9.
So I am confused whether one should tick Carbamazepine or Thiopental? But it seems like that the former is the correct answer.
8. (3)
Cushing's Triad
A triad of:
1. bradycardia
2. respiratory depression
3. hypertension
is called Cushing's triad (sometimes called Cushing's reflex or Cushing's response).
While the mechanism of Cushing's triad remains controversial, many believe that it relates to brainstem compression. The presence of this response is an ominous finding that requires urgent intervention.
Ref: Kaye, AH. Brain Tumors: An Encyclopedic Approach, 2 ed, Churchill Livingstone, New
York, 2001:205.
9. (4)
Systemic secondary injury to brain:
Well Hypothermia to certain extent protects brain by reducing metabolic processes, so it
(Looking at other options) is not logical that it might play a major role in injuring it.
10. (4)
Neostigmine antagonizes
Ref: KDT 3/E 86/P
11. (1)
Ref: Ganong 17/e 609/p
12. (4)
All of the following is used for treating hyperkalaemia,
1. Calcium gluconate
2. Sod. bi carb.
3. intravenous infusion of glucose with insulin
Intracellular movt of potassium is mediated by beta adrenergic receptors…so beta blockers stop this movt and raise serum potassium levels
- Dr. Vaibhav Sahni (S.R. Medicine, MAMC)
13. (1)
Ref: Harrison’s 16/e 1825/p
14. (1)
Coronary blood flow:
directly related to perfusion pressure and inversely related to resistance just like any blood flow pressure increases and resistance decreases flow.
- Dr. Vaibhav Sahni
15. (1) ?
Most significant adverse effect of ACE inhibitor is:
1. Hypotension
2. Hypertension
3. Hypocalcaemia
4. Hypercalcaemia rate answer is hyperkalemia
I don’t understand what hypercalcemia rate means. ACE inhibitors cause hypotension but very rarely…they may however cause first dose hypotension sometimes. Hypocalcemia or hypertension is not possible
- Dr. Vaibhav Sahni
16. (2)
Ref: KDT 3/e 207/p
17. (4)
Ref: KDT 5/e 164/p
18. (2)
- Dr. Anubhav Vindal
19. (1)
- Dr. Anubhav Vindal
20. (1)
- Dr. Anubhav Vindal
21. (3)
- Dr. Anubhav Vindal
22. (3)
A 40 yr old female patient presented with dysphagia to both liquids and regurgitation solids and for 3 months the dysphagia was non progressive, what is the most likely diagnosis is Achalasia cardia because dysphagia to both liquids nad solids suggests a motility disorder, not a structural one
- Dr. Vaibhav Sahni
23. (4)
- Dr. Ashwini Sethi (S.R. E.N.T., MAMC)
24. (3)
A 15 yr old boy presented with 1 d history of bleeding gum, subconjuctival bleed and the purpuric rash. Investigation revealed the following results:
Hb-6.4, TLC-26,500, Platelets-35,000,PT-20s with control of 13s, PTT-50s and fibrinogen 10mg/dl. Peripheral smear suggestive of AML. What is the most probable diagnosis?
Investigations suggests disseminated intravascular coagulopathy (DIC) – a typical presentation of promyelocytic leukemia.
- Dr. Vaibhav Sahni
25. (1)
Ref: Saini 2/e 7.5/p
26. (3)
Ref: Saini 2/e 6.26/p
27. (2)
pH=-log[H+]
28. (3)
Ref: Saini 2/e 9.71/p
29. (3)
Ref: Ananthnarayan 5/e 286/p
30. (2)
Homocysteine is an a.a. associated with Atherosclerosis
Ref: Kilmer McCully: pioneer of the homocysteine theory. Lancet 1998 352: 1364.
31. (4)
Ref: Robbin’s 5/e 300/p
32. (3) ?
Most of the searches landed me up into Hydrogen peroxide being a second messenger [Plant Cell, Vol. 13, 179-191, January 2001, Copyright © 2001, American Society of Plant Physiologists, Hydrogen Peroxide Acts as a Second Messenger for the Induction of Defense Genes in Tomato Plants in Response to Wounding, Systemin, and Methyl Jasmonate Martha L. Orozco-Cárdenasa, Javier Narváez-Vásqueza, and Clarence A. Ryana ].
Amongst the examples, I feel it should be Calcium. The article [Published 5 July 2004. doi:10.1083/jcb.200310145 JCB, Volume 166, Number 1, 111-119 Extracellular calcium acts as a "third messenger" to regulate enzyme and alkaline secretion, Rosa Caroppo1, Andrea Gerbino1, Gregorio Fistetto1, Matilde Colella1,2, Lucantonio Debellis1, Aldebaran M. Hofer2, and Silvana Curci1,2] says it acts as third messenger but if we take the definition, "Second messengers are molecules that relay signals received at receptors on the cell surface — such as the arrival of protein hormones, growth factors, etc. — to target molecules in the cytosol and/or nucleus. " then Calcium becomes an important Secondary messenger.
33. (2)
A != T && C != G
34. (4)
This is a debatable question though, because we never know how a mutation in intronic region affect the whole process (it might be a regulatory region or a splice site controller?) Anyways since we are appearing in medical entrance and not biotechnology one, we can safely go for the option (4)!
35. (1)
Ref: Park 18/e
36. (3)
Ref: Park 18/e 651/p
37. (3)
We are asked here to calculate the Negative predictive value.
[(Not Diseased)*(Specificity)]/[(Not Diseased)*(Specificity)
+ (Diseased)*(1-Sensitivity)]
[70*0.8]/[70*0.8+30(1-0.9)] =~ 95%
Ref: Harrison’s 14/e 10/p
38. (4)
Ref: Mahajan 6/e 11/p
39. (2)
Ref: Park 14/e 482/p
40. (1)
Ref: Park 14/e 480/p
41. (4) ?
Ref: Park 14/e 37/p
42. (4)
Ref: Ananthnarayan 5/e 481/p
43. (1)
Ref: Ananthnarayan 5/e 320/p
44. (2)
Ref: Ananthnarayan 5/e 320/p
45. (2)
Ref: Park 14/e 406/p
46. (2)
Ref: Park 18/e 241/p
47. (1)
48. (3)
Dr. Puneet Setia (S.R. Forensic Medicine, PGI Chandigarh)
49. (4)
Dr. Rahul Malhotra (S.R. Pulic Health, MAMC)
50. (1)
Ref: CMDT 2000/y 197/p
51. (2)
Ref: Park 14/e 347/p
52. (4)
Ref: Park 14/e 350/p
53. (4)
Ref: Park 14/e 15/p
54. (1)
Ref: Ananthnarayan
55. (4)
Ref: Park 14/e 111/p
56. (1)
Ref: Taber’s medical dictionary
57. (1)
Chancre redux I found out is another name for early relapse of syphilis
- Dr. Vaibhav Sahni
58. (2)
Max Joseph's space is linked to Lichen Planus.
Ref: Phd thesis of Laeijendecker, Proefschr on Lichen Planus.
59. Ivermectin is used in treating Scabies.
Ref: Prescrire Int. 2002 Oct;11(61):137-40; Ivermectin: new indication. Oral treatment of scabies: simple and effective.
60. (2)
Ref: Harrison’s 14/e 1016/p
61. (1)
Following is not used for treatment of typeII lepra reaction:
1. Chloroquin
2. Thalidomide
3. Cyclosporine
4. Corticosteroids
All others have an anti-inflammatory action and are used
- Dr. Vaibhav Sahni
62. (1)
Lepramin test is a test to measure cell mediated immunity. It just suggest whether the pt is immunocompetent or not. A lepramin negative pt develops the severe lepromatous leprosy and a lepramin positive one develops tuberculoid leprosy. This test cannot be used to diagnose leprosy.
- Dr. Vaibhav Sahni
63. (2)
Ref: Harrison’s 14/e 298/p
64. (2)
Ref: Maheshwari 3/e 81/p
65. (2)
Presentation suggests mononeuritis multiplex, nephritic syndrome , a young male----all typical of PAN
- Dr. Vaibhav Sahni
66. (4)
All of the following is used for giving traction, EXCEPT:
>1. Steinmann's Pin
>2. Kirschner's Wire
>3. Bohler's Stirrup
>4. Rush Pin*
- Dr. Ankur Gupta (S.R. Orthopaedics, RML)
67. (4)
All of the following are compilation of supracondylar fracture of
>humerus in children, except:
>1. Compartment syndrome
>2. Myositis ossificans
>3. Malunion
>4. Non union*
- Dr. Ankur Gupta
Ref: Maheshwari 2/e 84/p
68. (4)
Lesion associated with recurrent dislocation of shoulder include all,
>EXCEPT:
>1. Hill-Sach's lesion
>2. Bankart's lesion
>3. Capsular laxity
>4. Supraspinatous tear*
- Dr. Ankur Gupta
Ref: Maheshwari 2/e 74/p
69. (4)
All of the following are the cause of sudden increase in pain in
>osteochondroma, except:
>1. Sarcomatous change
>2. Fracture
>3. Bursitis
>4. Degenerative changes*
70. (3)
Dr. Anubhav Vindal
71. (2) ?
# The upper division of the oculomotor nerve (cranial nerve III) innervates the superior rectus and the levator palpebrae superioris muscles.
# The lower division of cranial nerve III innervates the inferior rectus, medial rectus, and inferior oblique muscles. The nerve to the inferior oblique muscle enters the muscle laterally at the junction of the inferior oblique and inferior rectus muscles.
# The trochlear nerve (cranial nerve IV) supplies the superior oblique muscle. The nerve to the superior oblique muscle enters the muscle approximately one third of the distance from the origin to the trochlea.
# The abducens nerve (cranial nerve VI) supplies the lateral rectus muscle.
# The parasympathetic innervation to the pupillary sphincter and ciliary muscle travels with the nerve to the inferior oblique muscle. The parasympathetics may be injured during inferior oblique surgery or orbital floor surgery.
Ref: http://www.emedicine.com/neuro/topic636.htm
And http://anesthesiologyinfo.com/articles/12092002.php says that “Retrobulbar block is aimed at blocking the ciliary ganglion, ciliary nerves, and cranial nerves II, III and VI. Cranial nerve IV is not affected since it lies outside the muscle cone. When the block is performed, the local anesthetic is delivered within the muscle cone itself.”
If we combine the above two we can see that superior oblique supplied by Cr. N. IV will not be much affected.
72. (2) or (4)?
For PHPV, prognosis is usually not good.
Ref: Trans Am Ophthalmol Soc. 1997;95:487-549. Persistent hyperplastic primary vitreous: diagnosis, treatment and results. Pollard ZF.
But one of my friend says answer can be (4) also, because it is asssosiated with microphthalmos.... not exophthalmos
- Dr. Pankaj Mehta
73. (3)
Panretinal photocoagulation is used for treating iris neovascularisation.
Ref: Ophthalmology. 1981 Nov;88(11):1102-6. A grading system for iris neovascularization. Prognostic implications for treatment.
74. (1)
- Dr. Pankaj Mehta
75. (2)
Ref: Neema 3/e 292/p
76. (3)
Ref: Robbin’s 5/e 236/p
77. (3)
Ref: Khurana 1/e 194/p
78. (2)
Ref: Khurana 1/e 144/p
79. (3)
Ref: Khurana 1/e 288/p
80. (2)
Ref: Khurana 1/e 289/p
81. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
82. (2)
Ref: Parikh 5/e 146/p
83. (2) ?
Dr. Anubhav Vindal
84. (4)
Ref: Reddy 16/e 146/p
85. (1)
Ref: Reddy 16/e 66/p
86. (1)
Ref: Reddy 24/e 125/p
87. (3)
Ref: Reddy 16/e 452/p
88. (4)
Ref: Robbin’s 5/e 1058/p
89. (4)
Ref: Harrison’s 14/e 2106/p
90. (4) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
91. (1)
- Dr. Anubhav Vindal
92. (3)
- Dr. Neeraj Srivastava (Resident CUNY, NYC) and Dr. Rachna Srivastava
93. (2)
Ref: Shaw’s 12/e 315/p
94. (2) ?
PREGNANCY INDUCED HYPERTENSION
37 WEEKS
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
95. (4) ?
ASHERMAN SYNDROME
(MISSED ABORTION)
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
96. (1) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
97. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
I think it is because of reflex hyperinsulinemia in the fetus because of hyperglycemia in mother…
98. (4) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236
99. (3)
Propofol . It is the recommended day care anaesthetic agent because of
Smooth induction , anti emetic and anti pruritic quality and smooth and
Pleasant clear headed recovery . The added mtp conundrum is a distraction at
Best .
Dr. Kapil Arya (S.R. Anaesthesia, LHMC)
100. (1)
- Dr. Neeraj and Rachna Srivastava
101. (4)
- Dr. Ashwini Sethi
102. (1)
- Dr. Ashwini Sethi
103. (2) ?
- Dr. Ashwini Sethi
But there is some controversy here as Harrison’s 14/e 2379/p puts Vertigo not as a typical feature.
104. (3)
- Dr. Ashwini Sethi
Ref: Harrison’s 14/e 944/p.
105. (1)
- Dr. Ashwini Sethi
106. (3)
- Dr. Neeraj and Rachna Srivastava
107. (2) ?
- Dr. Neeraj and Rachna Srivastava
But there is some controversy here because some of my friends say it is (3) Posterior urethral valve.
108. (1) ?
Transient synovitis (toxic synovitis) of the hip is characterized by all of the following, except:
4. The hip is typically held in adduction and internal rotation.
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
109. (1)
Ref: Harrison’s 14/e 2319/p
110. (4)
Ref: Harrison’s 14/e 1328/p
111. (4)
Ref: Robbin’s 5/e 598/p
112. (1)
Ref: Harrison’s 14/e 383/p
113. (4)
Ref: Harrison’s 14/e 1676/p
114. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
115. (4)
MAY BE 4 PROGNOSIS IN ARF DEPEND ON UNDERLYING Ds....BETTER WITH PRERENAL CAUSE THAN RENAL AND POST RENAL…
- Dr. Neeraj and Rachna Srivastava
116. (3)
Ref: Harrison’s 14/e 1629/p
117. (4)
- Dr. Anubhav Vindal
118. (3)
This is a case of amyloidosis.
- Dr. Vaibhav Sahni
119. (3)
Cytokeratin is an epithelial tissue marker. Only a carcinoma originates from epithelium.
- Dr. Vaibhav Sahni
120. (3) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
121. (3)
Ref: Robbin’s 5/e 1238/p
122. (4)
A differential diagnosis of lesion, histologically resemblin giant cell
>tumor in the small bones of hands or feet inclused all of the following
>EXCEPT:
>1. Aneurysmal bone cyst
>2. Fibrosarcoma
>3. Osteosarcoma
>4. Hyperparathyroidism*
- Dr. Ankur Gupta
123. (2)
Ref: Khurana 1/e 278/p
124. (1)
- Dr. Pankaj Mehta
125. (1) or (3)
Ref: Robbin’s 5/e 598/p says (1)
- Dr. Neeraj and Rachna Srivastava say (3)
126. (4)
- Dr. Neeraj and Rachna Srivastava
127. (2)
- Dr. Neeraj and Rachna Srivastava
128. (3)
46 XXY
Ref: Robbin’s 5/e 159/p
129. (4)
Ref: Robbin’s 5/e 635/p
130. (4)
Ref: Robbin’s 14/e 704/p
131. (3)
Acute leukemias show blasts in peripheral smear. Basophilia is a characteristic feature of CML.
- Dr. Vaibhav Sahni
132. (2)
Hb is normal so polycythemia is out. Normal TLC rules out leukemoid rxn. Also, this doesn’t suggest CML. Though platelets are only mildly raised I would still put my money behind thrombocythemia.
- Dr. Vaibhav Sahni
133. (3)
A 70 yr old with pathological fracture of femur. The lesion appears
>lytic on X-Ray film with a circumscribed punched out appearance. The
>curetting from the fracture site is most likely to show which of the
>following:
>1. Diminished and thinned trabecular bone fragments secondary to osteopenia
>2. Sheets of atypical plasma cells
>3. Metastatic prostatic adenocarcinoma*
>4. Malignant cell forming osteoid bone
- Dr. Ankur Gupta
134. (2)
Angiocentric lymphoma is a T-Cell lymphoma.
Ref: Journal of Clinical Pathology 2005;58:550-552 2005 BMJ Publishing Group Ltd & Association of Clinical Pathologists: Angiocentric immunoproliferative lesion and angiocentric lymphoma of lymph node in children. A report of two cases: R Drut and R M Drut.
135. (1)
Ref: Robbin’s 5/e 1137/p
136. (1)
Ref: Harrison’s 14/e 1593/p
137. (2)
It is a Vit K congener.
Ref: Harrison’s 14/e 745/p
KDT 3/e 544/p
138. (4)
- Dr. Divakar Sharma (S.R. Anesthesia, Safdarjung)
139. (2)or (4)
- Dr. Kapil Arya says (3)
Ref: KDT 3/e 315/p says (4)
140. (4)
- Dr. Kapil Arya says (3)
141. (1)
Ref: KDT 3/e 765/p
142. (1)
Imatinib inhibits Tyrosine kinase.
Ref: PNAS | September 20, 2005 | vol. 102 | no. 38 | 13622-13627: The kinase inhibitor imatinib mesylate inhibits TNF-{alpha} production in vitro and prevents TNF-dependent acute hepatic inflammation: Anna Maria Wolf , Dominik Wolf, Holger Rumpold, Susanne Ludwiczek, Barbara Enrich, Guenther Gastl, Guenter Weiss, and Herbert Tilg.
143. (2)
Letrozole is an aromatase inhibitor.
Ref: J Clin Oncol. 1998 Feb;16(2):453-61. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: double-blind randomized trial showing a dose effect and improved efficacy and tolerability compared with megestrol acetate. Dombernowsky P, Smith I, Falkson G, Leonard R, Panasci L, Bellmunt J, Bezwoda W, Gardin G, Gudgeon A, Morgan M, Fornasiero A, Hoffmann W, Michel J, Hatschek T, Tjabbes T, Chaudri HA, Hornberger U, Trunet PF.
144. (3)
Secondary leukemia is a common long term side effect of alkylating agents like cisplatin, doxorubicin, daunorubicin, idarubicin etc…
- Dr. Vaibhav Sahni
145. (4)
FOR REDUCING PULMONARY HYPERTENSION . IT IS A MEDICINE QUESTION . NITRIC OXIDE IS NO . NITROUS OXIDE , N2O IS AN ANAESTHETIC AGENT.
- Dr. Kapil Arya
146. (1)
CHEST WALL RIGIDITY
- Dr. Kapil Arya
147. (1)
Vanilloid receptors are activated by Pain.
" Capsaicin functions in nociception by binding to a specific receptor, called the vanilloid receptor (Caterina et al., 1997). "
Ref: Caterina, M.J., Schumacher, M.A., Tominaga, M., Rosen, T.A., Levine, J.D., and Julius, D. The Capsaicin Receptor: a heat-activated ion channel in the pain pathway. Nature 389: 816-24 (1997)
148. (2)
Ref: Ganong 17/e 177/p
149. (2)
Ref: Ganong 17/e 394/p
150. (2)
Ref: Ganong 20/e 431/p
151. (1)
Ref: Ganong 20/e 413/p
152. (1)
Ref: Ganong 20/e 413/p
153. (4) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
154. (4)
Ref: Ganong 17/e 224/p
155. (2)
Ref: Ganong 17/e 404/p
156. (1)
Acute dystonia Sort of hypersenstivity to anti dopaminergic ( mostly all anti psychotics) that is why responds to diphenhydramine and no loss of consciousness.
- Dr. Jatan Parmar (Resident Psychiatry, UK)
157. (2)
Too much anti dopaminergic and due to this very high acetylcholine (see saw with dopamine in the motor control system) leading to muscular rigidity (actually leading to muscle breakdown and high CPK) and labile blood pressure ( inc. OR decrease) Life threatening emergency. Treatment includes supportive measures like controlling temp and blood pressure and also centrally acting muscle relaxants commonly Dantrolene intramuscularly.
- Dr. Jatan Parmar
158. (3)
- Dr. Anubhav Vindal
Ref: Harrison’s 14/e 161/pn
159. (4)
Agoraphobia ( which actually means fear of open spaces) includes fear and subsequent avoidance of crowded places like public transport. It can be with or without panic disorder, in this case it is classically described with it.
- Dr. Jatan Parmar
160. (1)
Ref: Saini 2/e 10.55/p
161. (1)
Ref: Ananthnarayan 5/e 574/p
162. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
163. (3) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
164. (3) ?
165. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
166. (4)
Blasts and mediastinal LN suggest childhood ALL which is a Bcell malignancy.
- Dr. Vaibhav Sahni
167. (2)
Presentation suggests CHF – a common complication of doxorubicin.
- Dr. Vaibhav Sahni
168. (1)
Nodular growth in sunexposed areas especially the face and pearly appearance is characteristic of basal cell carcinoma.
- Dr. Vaibhav Sahni
169. (3)
This is a presentation of pancoasts tumour- seen in mostly SCC, can also be seen in small cell ca. Adenocarcinoma is usually central and does not have this complication.
- Dr. Vaibhav Sahni
170. (2)
>A 15 yr old boy is injured while playing cricket. X-Ray of leg rule out
>a possible fracture. The radiologist reports the boy has and evidence of an
>agressive bone tumor with both bone destruction and soft tissue mass. The
>bone biopsy reveals a bone cancer with neural differentiation. Which of the
>following is most likely diagnosis:
>1. Chodroblastoma
>2. Ewing's sarcome*
>3. Neuroblastoma
>4. Osteosarcome
171. (2)
- Dr. Anubhav Vindal
172. (2) ?
173. (2)
Ref: Robbin’s 5/e 1137/p
174. (1)
Ref: NMS Anatomy 2/e 529/p
175. (1)
Ref: Robbin’s 5/e 857/p
176. (2)
- Dr. Anubhav Vindal
177. (2)
Ref: Khurana 1/e 8/p
178. (3)
- Dr. Anubhav Vindal
179. (2)
Ref: Harrison’s 14/e 745/p
180. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
181. (2)
Ref: Ananthnarayan 5/e 385/p
182. (4)
Gram positive cocci in clusters and alpha hemolysis suggests staph aureus. It is commonly resistant to penicillin group but sensitive to methicillin group i.e. oxacillin, cloxacillin, etc
- Dr. Vaibhav Sahni
183. (3)
Gram positive cocci in chains and catalase negative suggests streptococcus group. Now enterococcus is commonly resistant to most antibiotics in contrast to viridans and is a common cause of nosocomial sepsis in pts in ICU
- Dr. Vaibhav Sahni
184. (3)
Ref: Ananthnarayan 5/e 245/p
185. (4)
Ref: Harrison’s 14/e 995/p
186. (4)
Ref: Harrison’s 14/e 1036/p
187. (1)
Ref: Harrison’s 14/e 782/p
188. (2)
Ref: Ananthnarayan 5/e 272/p
189. (4)
Ref: Ananthnarayan 5/e 288/p
190. (3)
Ref: Ananthnarayan 5/e
191. (2)
No explanation for this , you have TO REMEMBER THE FEATURES OF DENERVATION AND OF MYOPATHY. Polyphasic waves is a feature of myopathy.
- Dr. Vaibhav Sahni
192. (1)
- Dr. Neeraj and Rachna Srivastava
193. (3)
Known side effect of topiramate……man no one knows why!
- Dr. Vaibhav Sahni
194. (4)
Ref: Reddy 16/e 425/p
195. (3)
All of these are ECG findings of PE. Sinus tachy is the earliest and most common sign. S1Q3T3 is the most specific.
- Dr. Vaibhav Sahni
196. (2) ?
Ref: http://www.aippg.net/forum/viewtopic.php?t=35236&start=16
197. (2)
This suggests acute polyneuropathy. Descending presentation is seen in botulism and diphtheria but papillary involvement is seen only in botulism
- Dr. Vaibhav Sahni
198. (3)
Weakness is seen in hypokalemia, hypocalcemia, hypomagnesemia, hypophosphatemia, hypercalcemia…not usually in sodium problems
- Dr. Vaibhav Sahni
199. (1)
Triphasic waves is a characteristic EEG pattern of hepatic enceph. Don’t ask me why!
- Dr. Vaibhav Sahni
200. (4)
Factor XIII action is to stabilize the clot formed initially. Fibrin lysis test is abnormal in its deficiency.
My Sincere thanks to Anubhav, Vaibhav, Neeraj, Rachna, Pankaj, Tulsi, Divakar, Kapil, Ashwini, Ankur, Puneet, Rahul, Jatan, Medical Books and The Internet!
- Ani
PS: The Scanned Question paper is available in the previous posting.
posted by Ani at 10:53 AM
0 comments
![]()